eISSN 2444-7986
DOI: https://doi.org/10.14201/orl.27724
CASE REPORT
UNUSUAL COMPLICATIONS OF ACUTE FRONTAL RHINOSINUSITIS. TWO CLINICAL CASES
Complicaciones raras de la rinosinusitis frontal aguda. Dos casos clínicos
Pedro SANTOS  ; João ALMEIDA ; Isabel CARVALHO ; Cecília SOUSA
; João ALMEIDA ; Isabel CARVALHO ; Cecília SOUSA
Centro Hospitalar e Universitário do Porto, Serviço de Otorrinolaringologia. Porto. Portugal
Correspondence: pedrosantos288@gmail.com
Reception date: November 14, 2021
Date of Acceptance: February 5, 2022
Publication date: March 9, 2022
Date of publication of the issue: September 30, 2022
Conflict of interest: The authors declare no conflicts of interest
Images: The authors declare that the images have been obtained with the patients’ permission
Rights policy and self-archive: the self-archive of the post-print version [SHERPA / RoMEO] is allowed
License CC BY-NC-ND. Creative Commons Attribution-Noncommercial-NoDerivate Works 4.0 International
University of Salamanca. Its commercialization is subject to the permission of the publisher
SUMMARY: Introduction: Acute frontal rhinosinusitis is defined as an acute infection of the frontal sinus. Spreading of this infection to surrounding structures is uncommon but, when present, carries significant morbidity and mortality. Description: In this case report, we present two unusual cases of frontal rhinosinusitis complications. Firstly, we describe a case of acute rhinosinusitis with orbital complications caused by a frontoethmoidal osteoma. In the second case, the infection extended to the underlying bone and through the skull causing osteomyelitis and focal meningitis complicated with an abscess. After appropriate treatment, both patients were free of infection at follow-up, without complications. Discussion: In the first case we presented, a frontoethmoidal osteoma gave rise to rhinosinusitis with orbital complications. These benign tumors rarely cause symptoms, but when large enough, sinus outflow can be blocked, making the osteoma clinically relevant. Osteomas can induce frontal rhinosinusitis, giving rise, among other conditions, to the development of orbital complications like periorbital cellulitis or the formation of a periorbital abscess. Diagnosis of osteoma is usually straightforward on computed tomography and surgical treatment is only indicated for large tumors, rapid growth, intracranial or orbitary extension. In the second clinical case, the infection extended to the underlying bone and through the skull causing osteomyelitis and focal meningitis with abscess formation. In this patient, a Draf Type IIa procedure was performed for the frontal abscess drainage, followed by proper antibiotic and anti-inflammatory therapy. Conclusions: Complications of frontal rhinosinusitis are uncommon but require immediate attention and aggressive treatment to avoid morbidity and mortality. In these cases, our patients were properly treated with good outcomes, avoiding potentially more dangerous complications.
KEYWORDS: frontal sinusitis; osteoma; Pott Puffy tumor
RESUMEN: Introducción: La rinosinusitis frontal aguda se define como una infección aguda del seno frontal. La propagación de esta infección a las estructuras circundantes es poco común, pero, cuando está presente, conlleva una morbilidad y mortalidad significativas. Descripción: En este reporte presentamos dos casos inusuales de complicaciones de rinosinusitis frontal. En primer lugar, describimos un caso de rinosinusitis aguda con complicaciones orbitarias por osteoma frontoetmoidal. En el segundo caso, la infección se extendió al hueso subyacente y a través del cráneo causando osteomielitis y meningitis focal complicada con un absceso. Tras el tratamiento adecuado, ambos pacientes quedaron libres de infección en el seguimiento, sin complicaciones. Discusión: En el primer caso que presentamos, un osteoma frontoetmoidal dio lugar a una rinosinusitis con complicaciones orbitarias. Estos tumores benignos rara vez causan síntomas, pero cuando son lo suficientemente grandes, el flujo de salida del seno puede bloquearse, lo que hace que el osteoma sea clínicamente relevante. De hecho, los osteomas pueden inducir una rinosinusitis frontal, dando lugar, entre otras condiciones, al desarrollo de complicaciones orbitarias como celulitis periorbitaria o formación de un absceso periorbitario. El diagnóstico de osteoma suele ser sencillo mediante tomografía computarizada y el tratamiento quirúrgico solo está indicado para tumores grandes, de crecimiento rápido, con extensión intracraneal u orbitaria. En el segundo caso clínico, la infección se extendió al hueso subyacente y a través del cráneo provocando osteomielitis y meningitis focal con formación de abscesos. En este paciente, se realizó un procedimiento Draf Tipo IIa para el drenaje del absceso frontal, seguido de una adecuada terapia antibiótica y antiinflamatoria. Conclusiones: Las complicaciones de la rinosinusitis frontal son poco frecuentes, pero requieren atención inmediata y un tratamiento agresivo para evitar la morbilidad y la mortalidad. En estos casos, nuestros pacientes fueron tratados adecuadamente con buenos resultados, evitando complicaciones potencialmente más peligrosas.
PALABRAS CLAVE: sinusitis frontal; osteoma; Pott Puffy
INTRODUCTION
Acute rhinosinusitis often follows an upper respiratory tract infection. It is estimated that only 0.5% to 2% of viral upper respiratory tract infections are complicated by bacterial infection. The prevalence rates for acute rhinosinusitis vary from 6% to 12% [1]. Regarding complications, epidemiological studies estimate an incidence of three complications from rhinosinusitis per million population per year [2].
When the infection involves the frontal sinus, it is defined as acute frontal rhinosinusitis and generally occurs as part of generalized acute rhinosinusitis [3]. Its complications result from progression of the infection outside the sinus, which is relatively rare. Most complications tend to occur in children and young adults because of their thinner sinus walls [3].
Typically, patients with frontal rhinosinusitis come to medical attention with malaise, frontal headache, and tenderness of the orbital margin [4].
The infection usually responds to antibiotherapy. However, it may spread to structures surrounding the sinus [eye, nearby blood vessels, brain, bone, and overlying skin] carrying with them significant morbidity and mortality [5].
Surgical management of frontal sinus pathology remains among the more challenging subjects in otolaryngology and represents one of the most interesting facets of surgical rhinologic practice, requiring a significant level of advanced surgical skills [4].
DESCRIPTION
CASE 1
A 40-year-old male patient, with a 1-year history of right-sided frontal pain, presented with a 3-week right ocular pain, swinging pyrexia, and eyelid swelling with erythema. There was no history of trauma, nasal surgery, or paranasal sinus infection.
Computed tomography (CT) of the paranasal sinuses revealed a swelling of the eyelid and adjacent preseptal soft tissues, not involving the deeper orbital structures. An extremely dense lesion, with 23 mm cranio-caudal and 18 mm transversal diameters, located in the right frontoethmoidal region was also highlighted, extending to the orbit without invading it (Figure 1).

Figure 1. Coronal CT scan showing the dimensions of the lesion.
These findings strongly suggested periorbital cellulitis and was decided to control the infectious process with intravenous antibiotics [ceftriaxone and clindamycin] and dexamethasone for a period of 7 days. After this time and given the fact that the patient still had mild complaints even after a complete course of medical therapy, an external osteoplastic approach combined with endoscopic right frontoethmoidectomy was performed.
The surgical team decided for an external approach to address the frontal segment of the lesion because it allowed for a wide exposure and better control of the whole tumor, which was in direct contact with the superior and medial wall of the orbit.
Perioperatively, from an endoscopic and direct visualization, an ivory-like, smooth, and bony mass was observed, without orbital invasion. Complete resection was achieved.
CASE 2
A 18-year-old male patient, without known diseases, presented with a slow growing frontal tumefaction with 1 month of evolution, in association with fever and severe headache. Fluctuant swelling of the frontal region was noticed (Figure 2).

Figure 2. Frontal Tumefaction.
CT demonstrated an anterior table defect of the frontal sinus bilaterally and a left subgaleal abscess and right epidural empyema with focal meningitis. The CT also showed bony destruction of the frontal sinus, indicating osteomyelitis (Figure 3).
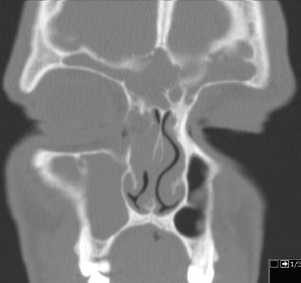
Figure 3. Coronal CT scan showing the occupation and destruction of the frontal sinus.
Due to a malfunction of the equipment at the time, MRI was not performed, and as it was an urgent surgical patient, the team opted to perform surgery solely with CT support.
The patient was submitted to endoscopic sinus surgery, through a Draf type IIa frontal sinusotomy, and received treatment post-surgically with intravenous antibiotics [ceftazidime, metronidazole and vancomycin] and dexamethasone for 4 weeks.
The results of the cultures revealed the presence of S. aureus spp.
Both patients were free of infection at 2 years of follow-up, without complications.
DISCUSSION
Complications of frontal rhinosinusitis are uncommon but require immediate attention and aggressive treatment to avoid morbidity and mortality [6].
In the first case presented, a frontoethmoidal osteoma gave rise to rhinosinusitis with orbital complications.
Approximately 3% to 4% of the general population have an osteoma in their paranasal sinuses, being the most frequent tumor of the sinonasal tract. These lesions are benign, often found incidentally in the paranasal sinus, more frequently the frontal sinus [80% of cases] [7]. Albeit rarely cause symptoms, these tumors can block sinus outflow when large enough, becoming clinically relevant [4].
About 4% to 10% of all osteomas cause clinical symptoms, which are usually related to the location, size, and growth pattern of the tumor [8].
The most commonly observed symptom is headache, especially located over the area of the osteoma [4]. Likewise, facial deformity, swelling or orbital symptoms are also reported [9].
Osteomas may originate frontal rhinosinusitis that may complicate, giving rise to the development of orbital complications like periorbital cellulitis or periorbital abscess. Patients with intraorbital complications present periorbital edema or erythema, pain, and visual complaints.
Diagnosis of osteoma is usually straightforward on CT, where they appear as rounded, bone-density mass lesions [10]. In the setting of high clinical suspicion of intraorbital and intracranial complications, MRI with and without intravenous contrast is most appropriate, due to its excellent soft-tissue resolution [11]. However, its limited availability and need for sedation in pediatric patients may impair its use. From a practical stand point, the fact that most of these complications are approached in emergency setting [where MRI is often not readily available] makes ceCT the most performed first-line imaging modality by far [12].
Regarding treatment, the general rule is clinical observation for asymptomatic osteomas, surgery is indicated only for large tumors, rapid growth, intracranial or intraorbital extension [6].
Nowadays, even osteomas with lateral extension into the frontal sinus can be removed endoscopically. However, when dealing with large-volume frontal osteomas, like in the first case presented, the need for external access may arise and the osteoplastic flap can be an option. With this technique, wide access to the frontal sinus can be attained. Allowing for radical tumor removal under direct visual control and is indicated in selected patients with orbit and anterior skull base extension [13].
In the second clinical case we presented, the infection extended to the underlying bone and through the skull causing osteomyelitis and focal meningitis complicated with the formation of an abscess.
The prevalence of skull osteomyelitis is 1.5% of all osteomyelitis and it has a mortality rate of 20-40% [14].
This is seen as a complication of acute and chronic frontal rhinosinusitis or trauma and is often associated with other intracranial complications. It is in fact a rare but serious complication, mostly seen in children and adolescents [15].
Due to the high risk of complications, early diagnosis and adequate surgical and antibiotic treatment are required. It is imperative to drain the subperiosteal pus and to establish drainage of the sinus. Presenting symptoms include frontal scalp swelling, headaches, fever, and frontal sinus tenderness [16].
Infection can potentially extend to both intracranial and extracranial spaces to cause periorbital and orbital cellulitis, meningitis, intracranial abscess, and sinus venous thrombosis [4].
While an urgent surgical evacuation of any intracranial complication collection is required, the surgical management of associated rhinosinusitis remains controversial [17].
In our center, we believe that the source of infection must be eradicated since delay in surgical intervention has been associated with prolonged hospitalization. In this patient, we used a Draf Type IIa procedure that consists of widening of the frontal outflow tract with the removal of cells, usually known as “uncapping the egg” technique [4].
In both cases presented, the patients were properly treated with good outcomes, avoiding potentially more dangerous complications.
CONCLUSIONS
Complications of frontal rhinosinusitis are uncommon but require immediate attention and aggressive treatment to avoid morbidity and mortality. In these cases, our patients were properly treated with good outcomes, avoiding potentially more dangerous complications.
REFERENCES
1.Fokkens WJ, Lund VJ, Hopkins C, Hellings PW, Kern R, Reitsma S, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology. 2020;Suppl S29:1–464.
2.Hansen FS, Hoffmans R, Georgalas C, Fokkens WJ. Complications of acute rhinosinusitis in The Netherlands. Fam Pract (Internet). 2012 Apr 1;29(2):147–53. Available from: https://doi.org/10.1093/fampra/cmr062
3.Wald ER. Sinusitis in children. Pediatr Infect Dis J. 1988 Nov;7(11 Suppl):S150-3.
4.Subtil J, Barros E. Rinologia Multidisciplinar. First Ed. Vilhena Mendonça MT, Arraiano Lopes M do C, editors. Lisboa: Edições Círculo Médico; 2019. 139–147 p.
5.Ozkurt FE, Ozkurt ZG, Gul A, Akdag M, Sengul E, Yilmaz B, et al. Managment of orbital complications of sinusitis. Arq Bras Oftalmol. 2014 Oct;77(5):293–6.
6.Chiu AG, Schipor I, Cohen NA, Kennedy DW, Palmer JN. Surgical decisions in the management of frontal sinus osteomas. Am J Rhinol. 2005;19(2):191–7.
7.Janovic A, Antic S, Rakocevic Z, Djuric M. Paranasal sinus osteoma: is there any association with anatomical variations? Rhinology. 2013 Mar;51(1):54–60.
8.Çelenk F, Baysal E, Karata ZA, Durucu C, Mumbuç S, Kanlıkama M. Paranasal sinus osteomas. J Craniofac Surg. 2012 Sep;23(5):e433-7.
9.Cheng K-J, Wang S-Q, Lin L. Giant osteomas of the ethmoid and frontal sinuses: Clinical characteristics and review of the literature. Oncol Lett. 2013 May;5(5):1724–30.
10.Erdogan N, Demir U, Songu M, Ozenler NK, Uluç E, Dirim B. A prospective study of paranasal sinus osteomas in 1,889 cases: changing patterns of localization. Laryngoscope. 2009 Dec;119(12):2355–9.
11.Dankbaar JW, van Bemmel AJM, Pameijer FA. Imaging findings of the orbital and intracranial complications of acute bacterial rhinosinusitis. Insights Imaging. 2015/08/08. 2015 Oct;6(5):509–18.
12.McCann MR, Kessler AT, Bhatt AA. Emergency radiologic approach to sinus disease. Emerg Radiol. 2021 Oct;28(5):1003–10.
13.Livaoĝlu M, Cakir E, Karaçal N. Large orbital osteoma arising from orbital roof: Excision through an upper blepharoplasty incision. Orbit. 2009;28(2–3):200–2.
14.Lang EE, Curran AJ, Patil N, Walsh RM, Rawluk D, Walsh MA. Intracranial complications of acute frontal sinusitis. Clin Otolaryngol Allied Sci. 2001 Dec;26(6):452–7.
15.Barros E. Complicações de Rinossinusopatia Aguda em Idade Pediátrica. In: Otorrinolaringologia Pediátrica. Edições Circulo Médico; 2016. p. 166–76.
16.Bambakidis NC, Cohen AR. Intracranial complications of frontal sinusitis in children: Pott’s puffy tumor revisited. Pediatr Neurosurg. 2001 Aug;35(2):82–9.
17.Svider PF, Sekhsaria V, Cohen DS, Eloy JA, Setzen M, Folbe AJ. Geographic and temporal trends in frontal sinus surgery. Int Forum Allergy Rhinol. 2015 Jan;5(1):46–54.